Incision and Drainage (I&D) is a fundamental surgical procedure addressing abscesses, involving a controlled incision to release accumulated pus and necrotic tissue.
Effective I&D management requires understanding abscess formation, appropriate patient preparation, and meticulous post-procedure care to minimize complications and ensure optimal healing.
Patients frequently require continued drain care post-discharge, highlighting the importance of comprehensive education regarding Jackson-Pratt (JP) drain management techniques.
What is Incision and Drainage?
Incision and Drainage (I&D) represents a core surgical technique employed to manage abscesses – localized collections of pus and necrotic tissue, often resulting from infection. Essentially, it’s a procedure where a skilled healthcare professional makes a deliberate incision through the skin to access the underlying abscess cavity.
The primary goal of I&D is to evacuate the accumulated purulent material, effectively removing the source of infection and promoting healing. This process not only alleviates local symptoms like pain, swelling, and redness but also prevents the infection from spreading to surrounding tissues.
Following the incision, the cavity is often gently debrided, removing any remaining debris or non-viable tissue. A drain, such as a Jackson-Pratt (JP) drain, may be placed to facilitate continued drainage and prevent re-accumulation of pus, particularly in larger or complex abscesses.
Indications for I&D
Incision and Drainage (I&D) is indicated when a patient presents with a palpable, fluctuant abscess – a clear sign of localized pus collection. Symptoms like significant pain, swelling, redness, and limitations in movement strongly suggest the need for intervention.
Specifically, I&D is appropriate for abscesses that are not responding to oral antibiotics alone. While antibiotics can help control the spread of infection, they often cannot penetrate the abscess cavity effectively to eradicate the source.
Furthermore, larger abscesses, those causing significant discomfort, or those posing a risk of spreading infection require prompt I&D. Abscesses resulting in systemic symptoms, like fever or chills, also necessitate immediate drainage to prevent sepsis.

Understanding Abscesses
Abscesses represent localized collections of necrotic tissue and pus, frequently caused by bacterial infection, manifesting as painful, swollen, and inflamed areas.
Abscess Formation and Pathophysiology
Abscess formation typically begins with a localized inflammatory response to a bacterial or, less commonly, a foreign body invasion. This initiates an influx of inflammatory cells – neutrophils, macrophages – to the site, attempting to contain and eliminate the offending agent.
As the inflammatory process continues, a capsule begins to form around the infection, walling it off from surrounding tissues. Within this capsule, pus accumulates, consisting of dead neutrophils, bacteria, cellular debris, and inflammatory byproducts.
The liquefaction of necrotic tissue contributes to the pus’s characteristic consistency. The body’s attempt to isolate the infection, while protective, creates a localized collection requiring intervention. Without drainage, the abscess can expand, causing increased pain, pressure on surrounding structures, and potentially leading to systemic infection.
Types of Abscesses Suitable for I&D
Incision and Drainage (I&D) is most effectively applied to localized abscesses exhibiting clear signs of pus accumulation, such as fluctuation on palpation, localized pain, redness, and swelling. Skin and soft tissue abscesses are frequently managed with I&D, representing a common presentation.
Perianal abscesses often require I&D due to their location and propensity for recurrence. Similarly, lacrimal gland abscesses, when associated with dacryocystitis, can benefit from controlled drainage.
Abscesses that are deeply seated, extensive, or associated with significant surrounding cellulitis may require broader surgical intervention alongside I&D. The decision to proceed with I&D is based on clinical assessment, imaging findings, and consideration of patient factors.
Contraindications to I&D
Incision and Drainage (I&D) is not universally applicable and presents contraindications requiring careful consideration. Abscesses located near vital structures – major blood vessels, nerves – pose increased risk and may necessitate alternative management strategies.
Immunocompromised patients, particularly those with uncontrolled diabetes or undergoing immunosuppressive therapy, may exhibit delayed wound healing and increased susceptibility to infection, potentially complicating I&D.
Patients with cirrhosis and ascites present unique challenges due to altered fluid balance and increased risk of bleeding. Furthermore, abscesses with extensive surrounding cellulitis or signs of systemic infection (sepsis) may require broader antibiotic therapy and surgical debridement rather than simple I&D.

Pre-Procedure Preparation
Thorough patient assessment, including medical history and physical examination, is crucial before I&D. Obtaining informed consent and gathering necessary equipment ensures a safe procedure.
Patient Assessment and History
A comprehensive patient assessment is paramount prior to performing an incision and drainage. This begins with a detailed medical history, focusing on immunocompromising conditions, such as cirrhosis or immunosuppression, as these factors significantly impact healing and infection risk.
Specifically inquire about current medications, particularly anticoagulants or steroids, which may influence bleeding or wound healing. A thorough physical examination should pinpoint the abscess location, size, and surrounding tissue characteristics – noting redness, warmth, and tenderness.
Assess for signs of systemic infection, like fever or chills. Document any prior I&D procedures and their outcomes. Understanding the patient’s overall health status and the abscess’s specific presentation guides appropriate procedural planning and risk mitigation.
Informed Consent
Obtaining informed consent is ethically and legally essential before proceeding with an incision and drainage. The discussion must clearly articulate the procedure’s purpose – to drain an abscess and remove infected material – alongside potential benefits like pain relief and infection resolution.
Patients need to understand the inherent risks, including bleeding, hematoma formation, recurrence of the abscess, and the possibility of infection, even with MRSA. Explain anesthesia options and their associated risks.
Detail post-operative care requirements, such as wound packing, drain management (if applicable), and pain control. Ensure the patient has ample opportunity to ask questions and express concerns before signing the consent form, demonstrating their voluntary agreement.
Equipment and Supplies
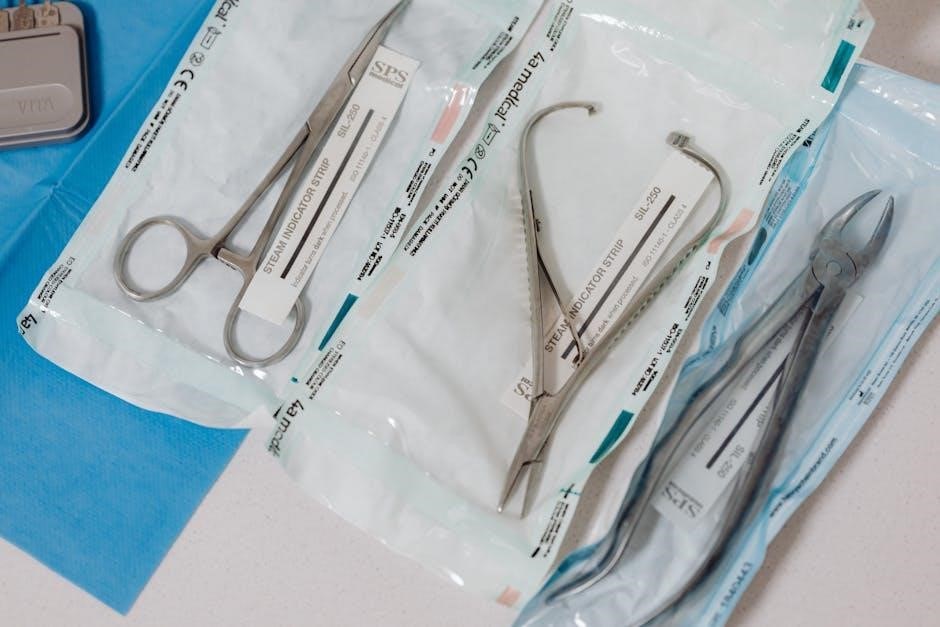
Essential equipment for incision and drainage includes sterile gloves, drapes, and gowns to maintain a sterile field. Antiseptic solution (like chlorhexidine or povidone-iodine) is crucial for skin preparation. Local anesthetic (lidocaine with or without epinephrine) is needed for pain control.
Instruments should encompass a scalpel with appropriate blades, forceps (both toothed and smooth), a hemostat, and a drainage system – potentially a Jackson-Pratt or Hemovac drain – depending on the abscess size and location.
Additional supplies include sterile gauze, wound packing material, suture material (if needed for closure), and appropriate dressings. Ensure availability of equipment for potential complications, like bleeding control supplies.
The Incision and Drainage Procedure
I&D involves carefully creating an incision over the abscess, following natural skin creases when possible, to facilitate pus drainage and debridement of necrotic tissue.
Anesthesia Options
Local anesthesia is frequently sufficient for smaller, superficial abscesses, offering a quick and straightforward approach. Typically, lidocaine with or without epinephrine is infiltrated directly into the surrounding tissue, providing effective pain control during the I&D procedure.
For larger or deeper abscesses, or in patients with significant pain or anxiety, regional anesthesia – such as a digital block or a field block – may be considered. These techniques provide broader and more prolonged pain relief.
In certain cases, particularly with extensive or complex abscesses, or if the patient requires immobilization, sedation or general anesthesia might be necessary. This decision is made based on the abscess location, patient’s medical history, and the surgeon’s judgment.
Careful assessment of the patient’s allergies and medical conditions is crucial before selecting any anesthetic option.
Incision Technique – Location and Depth
Incision placement should ideally follow the lines of skin tension and avoid crossing major blood vessels or nerves to minimize complications. Selecting a natural skin crease in a dependent area is often preferred for optimal drainage.
The incision length is determined by the abscess size, generally starting with a shorter incision that can be extended if needed. The goal is to provide adequate access for drainage and debridement.
Incision depth must be sufficient to reach the abscess cavity, but avoid unnecessary deep dissection. The point of maximal fluctuation often indicates the optimal entry point.
Careful dissection through the subcutaneous tissue is performed, respecting tissue planes, until the abscess cavity is identified and accessed.
Drainage of Pus and Debridement
Once the abscess cavity is accessed, pus and necrotic debris are gently evacuated. Copious irrigation with sterile saline solution helps remove residual contaminants and ensures thorough cleansing of the wound.
Debridement, the removal of non-viable tissue, is crucial for promoting healing and preventing re-accumulation of infection. This involves carefully excising any dead or damaged tissue within the abscess cavity.
Ensure complete evacuation of all loculations within the abscess. Exploration with a blunt instrument can help identify and break down any remaining pockets of infection.
Following thorough drainage and debridement, a drain may be placed to facilitate continued removal of any residual fluid and prevent premature closure.

Post-Procedure Care
Post-I&D care focuses on wound management, drain maintenance if present, and effective pain control to promote healing and prevent complications like infection.
Wound Packing and Dressing
Wound packing after I&D is crucial, especially for larger abscess cavities, to prevent premature closure and allow continued drainage of residual fluid or pus. Packing materials, like gauze, conform to the wound shape, filling dead space and promoting healing from the inside out.
The packing should be loose enough to avoid pressure but firm enough to maintain its position. Dressings applied over the packing must be occlusive to maintain a moist wound environment, facilitating granulation tissue formation.
Regular dressing changes, guided by drainage amount and wound appearance, are essential. Patients should be educated on proper dressing techniques and signs of infection, such as increased pain, redness, or purulent discharge. Consistent monitoring and appropriate wound care significantly reduce the risk of complications and promote optimal recovery.
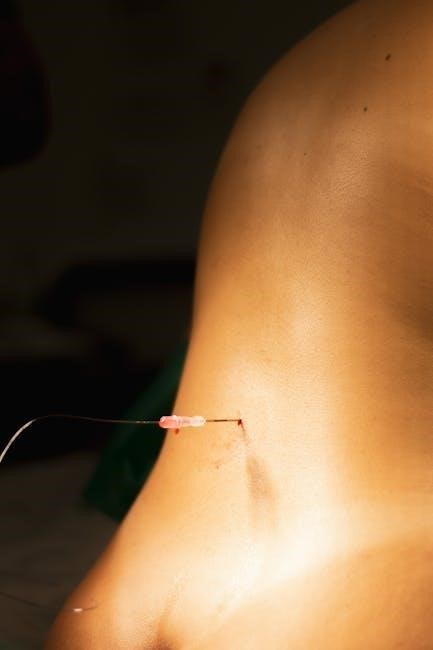
Drain Management (Jackson-Pratt, Hemovac)
Jackson-Pratt (JP) drains and Hemovacs are commonly used after I&D to remove accumulated fluid, preventing re-accumulation and promoting wound healing. JP drains utilize negative pressure, while Hemovacs rely on suction and a collection reservoir.
Patients discharged with drains require detailed education on proper care. This includes emptying the reservoir when half-full (Hemovac) or according to output (JP), maintaining drain site cleanliness, and recognizing signs of infection.
Drain removal is typically performed when output decreases significantly, indicating adequate healing. Healthcare providers assess the wound before removal, ensuring minimal leakage. Post-removal dressings are applied, and patients are monitored for any signs of fluid collection or complications.
Pain Management
Post-I&D pain is common and requires a multimodal approach. Initial management often involves over-the-counter analgesics like acetaminophen and ibuprofen, adjusted based on pain severity. For moderate to severe pain, opioid analgesics may be prescribed, with careful consideration of potential side effects and dependence.
Non-pharmacological methods, such as ice packs and proper wound positioning, can also contribute to pain relief. Patients should be educated on the importance of taking analgesics as prescribed and reporting any uncontrolled pain.
Effective pain control is crucial for patient comfort, wound healing, and adherence to post-operative care instructions, ultimately improving overall outcomes.

Potential Complications
I&D carries risks including infection – notably MRSA – bleeding, hematoma formation, and abscess recurrence, demanding vigilant monitoring and prompt intervention.
Infection (Including MRSA)
Post-I&D infection remains a significant concern, potentially stemming from the original abscess organism or introducing new pathogens during the procedure. Methicillin-resistant Staphylococcus aureus (MRSA) poses a particularly challenging threat, often requiring specific antibiotic regimens.
A case study illustrates a MRSA infection occurring two years after cosmetic surgery, manifesting as non-healing wounds. Signs of infection include increased pain, redness, swelling, purulent drainage, and systemic symptoms like fever.
Prophylactic antibiotics are generally not routinely recommended for simple I&D, but are crucial if there’s surrounding cellulitis, systemic illness, or immunocompromise. Culture and sensitivity testing of the abscess drainage guide appropriate antibiotic selection, especially when MRSA is suspected.
Bleeding and Hematoma Formation
Bleeding is a potential complication following incision and drainage (I&D), particularly in patients with underlying coagulopathies or those on anticoagulant medications. Careful hemostasis during the procedure – meticulous attention to blood vessel ligation or cauterization – is paramount to minimize this risk.
Hematoma formation, a localized collection of blood, can occur even with careful technique. Small hematomas typically resolve spontaneously, but larger ones may require aspiration or further surgical intervention.
Post-operative pressure dressings help to control bleeding and prevent hematoma development. Patients should be instructed to monitor the wound site for signs of excessive bleeding or rapidly expanding hematoma, and seek prompt medical attention if these occur.
Recurrence of Abscess
Abscess recurrence following incision and drainage (I&D) represents a significant concern, often indicating incomplete drainage or an underlying source of infection; Thorough debridement of all necrotic tissue and identification of the causative organism are crucial preventative measures.
In cases of recurrent abscesses, especially those linked to specific locations like the perianal region, investigation for underlying factors – such as fistulas or foreign bodies – is essential.
Patients should be educated on proper wound care and signs of re-accumulation of pus. Addressing contributing factors, like immunocompromise, can also reduce recurrence rates and improve long-term outcomes.

Specific Abscess Locations & I&D Considerations
I&D techniques vary based on abscess location; perianal, skin/soft tissue, and lacrimal gland abscesses each require tailored approaches for optimal drainage and healing.
Perianal Abscesses
Perianal abscesses commonly arise from infection of anal glands, presenting with localized pain, swelling, and often fever. I&D is the primary treatment, typically performed in the operating room under local anesthesia.
The incision is strategically placed to align with the anal canal, ensuring complete drainage and minimizing the risk of fistula formation. Thorough debridement of necrotic tissue is crucial. Post-operatively, wound care involves sitz baths and local analgesics.
Careful consideration must be given to potential underlying causes, such as Crohn’s disease or immunosuppression. Recurrence is common, often necessitating further evaluation for a fistula-in-ano, which may require additional surgical intervention. Proper documentation of the procedure and follow-up are essential.
Skin and Soft Tissue Abscesses
Skin and soft tissue abscesses frequently present as painful, erythematous, and fluctuant masses. I&D is a mainstay of treatment, often performed in an outpatient setting. Incisions should follow skin tension lines whenever possible to optimize healing and minimize scarring.
Complete drainage and thorough debridement are vital, particularly if there’s concern for underlying cellulitis. MRSA is a common causative agent, necessitating consideration of antibiotic coverage based on local resistance patterns.
Post-procedure care includes wound packing, regular dressing changes, and monitoring for signs of recurrent infection. Patient education regarding proper wound care and potential complications is paramount for successful outcomes.
Lacrimal Gland Abscesses & Drainage
Lacrimal gland abscesses, though rare, require prompt attention due to their potential for vision compromise. Drainage can offer relief for patients experiencing dacryocystitis, minimizing the risk of lacrimal fistula formation. A retrospective analysis suggests effective outcomes with this approach.
Careful consideration of anatomical landmarks is crucial during I&D to avoid injury to surrounding structures. The procedure often involves a careful incision and drainage of the purulent material.
Post-operative monitoring for signs of infection or fistula development is essential. Antibiotic therapy is typically administered alongside drainage to address the underlying infection.

Special Populations
I&D in immunocompromised or cirrhotic patients demands heightened vigilance due to increased infection risk and potential complications like refractory ascites.
I&D in Immunocompromised Patients
In immunocompromised patients, incision and drainage of abscesses presents unique challenges due to impaired wound healing and a significantly elevated risk of disseminated infection. Conditions like HIV/AIDS, chemotherapy, or chronic steroid use weaken the body’s natural defenses, making these individuals particularly vulnerable to complications.
Aggressive surgical debridement is often necessary, alongside broad-spectrum antibiotic coverage, potentially including agents effective against opportunistic pathogens. Prolonged drain management may be indicated to ensure complete evacuation of infected material. Careful monitoring for signs of sepsis or worsening infection is crucial.
Consideration should be given to the patient’s underlying immune status when determining the appropriate post-operative care plan, emphasizing meticulous wound care and close follow-up to prevent recurrence or spread of infection.
I&D in Patients with Cirrhosis & Ascites
Patients with cirrhosis and ascites undergoing incision and drainage require specialized consideration due to altered physiology and increased surgical risks. Ascites creates a challenging surgical field, potentially increasing the risk of wound complications like infection and dehiscence.
Coagulopathy, common in cirrhosis, necessitates careful assessment and potential correction prior to the procedure. The build-up of fluid can also cause difficulty breathing, fatigue, and abdominal pain, impacting post-operative recovery.

Judicious fluid management and consideration of paracentesis to reduce ascites prior to I&D may be beneficial. Close monitoring for signs of spontaneous bacterial peritonitis (SBP) is essential, alongside appropriate antibiotic prophylaxis.
Documentation and Follow-up
Detailed charting of the I&D procedure, including findings, interventions, and drain details, is crucial. Scheduled follow-up appointments ensure proper wound healing and monitor for complications.
Charting the Procedure
Comprehensive documentation is paramount following an Incision and Drainage (I&D) procedure. The medical record should meticulously detail the patient’s presentation, including abscess location, size, and any associated signs of infection.
Specifically, record the anesthesia type used, the incision site and length, the amount and characteristics of the drained fluid (color, consistency, odor), and any debridement performed.
Note the type of drain placed – if applicable – such as a Jackson-Pratt or Hemovac, and document its initial output.
Any complications encountered during the procedure, like bleeding or difficulty accessing the abscess, must be clearly noted. Finally, include details regarding post-procedure wound care instructions provided to the patient and scheduled follow-up appointments.
Post-Procedure Follow-up Appointments
Scheduled follow-up is crucial after Incision and Drainage (I&D) to monitor healing and detect potential complications. Initial appointments, typically within 24-72 hours, assess wound appearance, drain output (if present), and signs of infection like increasing pain, redness, or fever.
Further appointments may be needed weekly until complete wound closure. These visits allow for dressing changes, drain removal (when appropriate), and evaluation for abscess recurrence.
Patients should be educated on recognizing infection symptoms and instructed to seek immediate medical attention if they arise.
Documentation of wound progress at each visit is essential, alongside reinforcement of proper wound care techniques.